


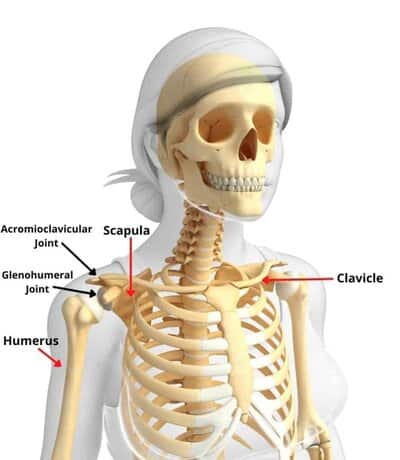
Basic Shoulder Anatomy
The shoulder is comprised of three bones moving together in unison.
Humerus (upper arm bone)
Scapula (shoulder blade)
Clavicle (collar bone)
This allows for increased freedom of movement for the arm so that it can raise overhead, behind your back, and across the body.
The shoulder is made up of three joints working together in unison.
Glenohumeral Joint
- Where the humerus meets the scapula (ball-in-socket joint)
Acromioclavicular Joint
- Where the clavicle meets the scapula (gliding-type joint)
Sternoclavicular Joint
- Where the clavicle meets the sternum (gliding-type joint)
As you can see, there are a lot of moving parts in the shoulder joint. This provides an immense amount of freedom of movement for the shoulder and arm, however, it also makes the shoulder joint inherently unstable. It requires the help of many soft tissues (labrum, ligaments, muscles, and tendons) to help to hold it together.
As a result, these bones and soft tissues can easily be injured in the form of dislocations, fractures, tears, sprains, and strains.
Now that we understand the basics behind the shoulder joint anatomy, let’s discuss the most common shoulder injuries that one may experience.
Rotator Cuff Tendinitis and Tears
Rotator cuff tendinitis is often the result of a typical muscle/tendon strain. The rotator cuff is a collection of four relatively small muscles that all come from the scapula and insert into the head of the humerus bone. If you haven’t yet read my article on Rotator Cuff Exercises for Beginners, you should do that now as it gives a much greater in-depth discussion on the rotator cuff.
The four muscles that make up the rotator cuff are the:
Supraspinatus
Infraspinatus
Teres Minor
Subscapularis

The primary purpose of the rotator cuff muscles is to help stabilize the shoulder while the arm is moving throughout space. These muscles attach to the top of the upper arm bone (called the humeral head) where they can optimally pull on it and hold it into the glenoid fossa (the area where the arm bone meets the shoulder blade).
The problem arises when these muscles are repetitively overworked and/or when there is a sudden strain placed upon one or more of them. Since they are small muscles, they can easily become inflamed (rotator cuff tendinitis) or even suffer a rotator cuff partial or full-thickness tear/s.
Rotator cuff-related pain is usually a dull, ache-type pain when the arm is at rest. Most people complain of increased shoulder pain when trying to sleep on that side at night. Additionally, the pain can be a sharp, stabbing-like pain with certain arm movements that cause activation of the injured rotator cuff muscle/s.
Treatment Options:
For most people with rotator cuff-related pain, the first step is to try physical therapy. Research has shown that physical therapy (PT) can significantly help reduce rotator cuff-related pain and improve functional outcomes for most individuals. Rotator cuff stretches should be initiated soon after the initial onset of shoulder pain is reported. This should gradually transition to rotator cuff strengthening exercises once the pain begins to decrease.
The individual should discuss the option of getting a corticosteroid injection with their doctor if the physical therapy exercises are not helping to reduce the shoulder pain, or if the person cannot tolerate physical therapy exercises because the shoulder pain is too severe. The corticosteroid injection has anti-inflammatory effects inside the joint. If an injection IS received, continue with physical therapy to see if the tolerance to PT activities improves.
If the pain has still not subsided significantly, then it is time for a referral to a shoulder specialist (likely an orthopedic surgeon).
A shoulder MRI (magnetic resonance imaging) will likely be ordered to determine the severity of the shoulder/arm injury and what structures are involved.
Depending on what the MRI finds, the orthopedic surgeon may recommend surgery. It is also possible to try a second corticosteroid injection with continued physical therapy if there are no rotator cuff tears or other significant injuries found on the MRI.
Sub-Acromial Impingement Syndrome (SAIS)
The subacromial space is the area directly underneath the Acromion bone in the shoulder. Think of the Acromion as the roof to the shoulder as it sits at the top and is relatively flat.

In those with healthy shoulders, the subacromial space is normally only 1 cm tall. It doesn’t take much in the form of capsular stiffness, muscle tightness, or poor coordination to close this space down quickly and cause pinching of the rotator cuff tendons within this space.
This pinching of the tendons is referred to as Sub-Acromial Impingement Syndrome. If this continues repetitively over time, it will lead to rotator cuff tendonitis/tears and/or Bursitis.
Treatment Options:
Physical therapy should be the first intervention for this condition as it will help to restore the proper shoulder mechanics and improve the muscle coordination of the joint.
The treatment intervention sequence will start with rotator cuff stretches immediately, and then gradually transition to rotator cuff strengthening as the pain decreases.
Shoulder Bursitis
A bursa is a fluid-filled sac that helps to pad the space between the bone and soft tissue. There is one located within the sub-acromial space along with the rotator cuff tendons. Typically the same aggravating activities such as repetitive reaching and lifting that causes rotator cuff-related pain will also simultaneously cause inflammation of the bursa, which is called bursitis.
Bursitis shoulder pain is also similar to rotator cuff-related pain in that it can be sharp, stabbing-type pain with arm movements and also a dull, ache the rest of the time.

Treatment Options:
Shoulder bursitis is treated initially with physical therapy exercises as bursitis and rotator cuff tendonitis/tears are expected to occur simultaneously. Again, a similar path of physical therapy for rotator cuff stretching and strengthening exercises, corticosteroid injection, MRI, surgery as described in the rotator cuff tendonitis/tears section would occur.
Glenoid Labrum Tears
The glenoid labrum is an oval-shaped ring of fibro-cartilage that encircles the outer edge of the glenoid fossa (the socket part of the ball-in-socket shoulder joint). The purpose of the labrum is to increase the depth of the socket to improve joint stability.

The labrum can easily be torn from the bone during high-velocity movements (i.e. throwing) or in the event of shoulder dislocation when the head of the humerus “pops out of the joint” either to the front (anterior dislocation) or to the rear (posterior dislocation).
Sometimes the labral tear also involves the biceps tendon, which is called a SLAP tear. If you’re familiar with baseball, then it’s likely that you have heard of a SLAP tear before as it is fairly common with throwing activities.

If we remember that a muscle inserts into a bone via a tendon; the biceps tendon blends into the top of the glenoid labrum at the 12 o’clock position. Repetitive pulling of the biceps tendon on its insertion point into the labrum can result in tearing of the labrum from the bone or even tearing of the biceps tendon itself.
This type of injury is called a SLAP tear (which stands for “superior labrum from anterior to posterior”). This simply describes that the tear occurs at the top of the labrum (superior) and runs from front to back (anterior to posterior).
Labral tears usually cause clicking or popping with arm movements and pain can be sharp, stabbing. During rest, the pain can be a dull, ache.
Treatment Options:
Glenoid tears can be persistent. This is especially true if the person continues to place high levels of stress on the labrum (i.e. if a pitcher continues to throw baseballs). Physical therapy should still be trialed as the rotator cuff can be strengthened to help stabilize the shoulder joint and allow the inflammation to decrease.
If the pain does not decrease, then an MR arthrogram (MRA) should be ordered. An MR arthrogram is different than a standard MRI. During the arthrogram, a dye (will be injected into the shoulder joint. If the dye leaks out of the joint via a tear in the labrum, the MRI will pick up on it and help to identify the location of the tear.
Depending on the needs of the person, a surgical labrum repair may be recommended by the orthopedic surgeon. Otherwise, continued physical therapy exercises will be ordered.
Frozen Shoulder (Adhesive Capsulitis)
Frozen shoulder is most easily described using a visualization. Imagine that the shoulder joint is wrapped in plastic wrap. The plastic wrap represents the fibrocartilagenous capsule that surrounds the joint. Then, if you took a heating gun and caused a shrink wrapping effect on the capsule, the whole capsule tightens and thickens up around the joint.

The shrink wrap effect is actually an inflammatory process that the body initiates. Science is not sure as to the true cause of the process yet, but there is some idea that is an overactive autoimmune response.
This is a very painful process for the individual as it is occurring gradually over time. Additionally, a noticeable and gradual loss of shoulder range of motion will occur. This phase is known as the “freezing phase.”
The freezing phase can last anywhere from 2-4 months in duration.

Eventually, the person will begin to notice that the gradual loss in shoulder range of motion will stop and the pain may decrease slightly. This new phase is called the “frozen phase.” I consider this phase as more of a plateau phase and it lasts anywhere from 2-4 months.
Finally, the scale will finally tip, and a slow, but gradual improvement in shoulder range of motion and decrease in pain will begin to occur. This last phase is referred to as the “thawing phase.” Again, it can last anywhere from 2-4 months.
Treatment Options:
It is imperative to have early identification during the initial freezing phase. Medical research has confirmed that, in most cases, the first intervention should be to receive a corticosteroid injection into the shoulder joint. This will prevent the inflammatory process from progressing and it can help limit the overall severity/duration of the process.
Physical therapy Frozen Shoulder Exercises will focus on maintaining shoulder range of motion and general function during this time.

Shoulder Dislocations
Shoulder dislocations are never a fun experience for anyone. They are usually the result of blunt force trauma that causes the head of the humerus to “pop out of the join.” This can occur to the front (anterior dislocation) or to the rear (posterior dislocation). It just depends on which direction the force came from when it occurred.
Most dislocations happen to a younger population (and males more often than females) as younger males tend to participate in the riskiest activities.

Remember from the Gelonoid Labrum section above that shoulder dislocations will likely also result in a simultaneous labral tear.
Treatment Options:
After the initial injury, you will likely be placed in a sling for 2-4 weeks. Physical therapy should be initiated for a safe range of motion activities to prevent stiffness and muscle atrophy (weakness).
Research has shown that surgical intervention is likely the best treatment for long-term stabilization of the joint in younger people. Once the shoulder has been dislocated once, the joint becomes chronically unstable. Recurrent dislocations are much more likely afterward due to the higher demands that younger people will likely place the shoulder in throughout the remainder of their lives.
A much more in-depth discussion should be had with older folks who dislocate their shoulders. They are much less likely to participate in activities that will require dynamic stability of the shoulder. If this is the case, then they would most likely be okay without requiring surgical stabilization of the joint.
Either way, physical therapy exercises would be beneficial to help strengthen the rotator cuff muscles and retain a functional range of motion of the shoulder.
Shoulder Osteoarthritis
As people age, gradual joint degeneration can and will occur. This degenerative process is called osteoarthritis. It is a natural process. The rate of degeneration depends on a lot of factors such as general health, previous injuries to that area, etc.
Osteoarthritis pain is typically reported as a toothache, dull, throbbing type of pain.
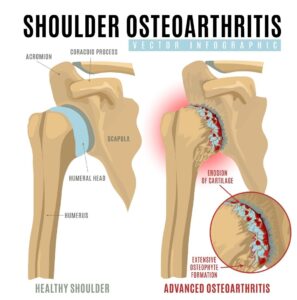
Sometimes osteoarthritis can lead to the development of bone spurs. Unfortunately, one of these areas is located on the bottom side of the Acromion bone. Remember that the Acromion is the “roof” to the shoulder joint.
In the medical world, we call this bone spur a “hooked Acromion.” In an x-ray, it appears as though the bottom of the Acromion has grown a beak. Since the Sub-acromial space is only normally 1 cm wide, the hooked part of the bone can gradually cause fraying or tearing of the rotator cuff muscles/tendons that lie underneath it.
It is commonplace that if a hooked Acromion is located by an orthopedic surgeon during any shoulder arthroscopic procedure, the bone spur will likely be shaved down to a flat surface in a procedure called subacromial decompression.
Treatment Options:
Physical therapy exercises are the best bet with the early stages of osteoarthritis. Exercises will focus on achieving optimal shoulder mechanics, strength, and preservation.
There are some injections that may be considered for osteoarthritis pain relief. Hyaluronic acid injections (HA injections) may allow for improved joint preservation. Other injection considerations (though they are still in the research phases) are stem cells and PRP (platelet-rich plasma).
Later stages of osteoarthritis will likely require shoulder replacement surgery. Either a total shoulder arthroplasty (TSA) or reverse total shoulder arthroplasty (RSA) will be performed depending on the quality of the rotator cuff muscles/tendons.

Physical therapy will typically start within a couple of weeks after these surgeries in order to prevent joint stiffness and return the patient to optimal function.
AC Joint Sprain (Acromioclavicular Joint)
The AC Joint (Acromioclavicular joint) is the joint where the Clavicle meets the Acromion part of the Scapula bone. These two joints are held together via 2 ligaments.
This joint is most often injured when an individual incurs a blunt force against the outside of the shoulder, or a force up through the humerus bone (i.e. fall onto an elbow after slipping on a patch of ice).
Depending on the severity of the force, the ligaments holding the joint together may either be simply stretched or even possibly torn. This injury is referred to as an AC Joint Sprain.

Treatment Options:
Physical therapy can help the AC Joint Sprains by improving pain-free shoulder range of motion as well as teaching the individual taping techniques to assist in AC joint stabilization while waiting for the ligaments to heal.
Surgery for this injury is only considered in severe situations.
Humerus Fractures
I think it’s obvious to say that humerus fractures typically require some form of blunt force trauma. I can’t think of how many times that I’ve treated these injuries in patients who have slipped or tripped and fallen onto their shoulders. An individual who has suffered a Humerus fracture will need immediate medical care, so Call 911 or take them to the Emergency Department at a local hospital.
Treatment Options:
The orthopedic surgeon will take x-rays and assess if the fracture site is considered to be “displaced” or “non-displaced.”
If the fracture is considered displaced, then surgical intervention will be required and an open-reduction interval fixation (ORIF) procedure will likely be performed.

If the fracture is considered non-displaced, then physical therapy will be ordered to help restore shoulder range of motion and strength.
During physical therapy, expect this to be painful as your physical therapist will need to stretch the shoulder gradually back to its normal range of motion. I have experienced good success though with getting these patients back to a functional range within 8 weeks of therapy, though.



